Rory Hearne: Health inequalities affect children in a number of ways. One measure of health inequality is waiting lists for various forms of treatment or assessment in our public hospital system. The recent HSE figures show that the trend in waiting lists is worsening for children in Ireland. The numbers of children waiting to be seen in hospital day cases, for example, has risen by a third (33.7%) in just over a year (from December 2014 to March 2016).
Meanwhile the number of children on inpatient (often surgery) waiting lists has increased by 18% in the same period.
So while we are commemorating 100 years since the Proclamation of the Irish Republic that declared “its resolve to pursue the happiness and prosperity of the whole nation and of all its parts, cherishing all of the children of the nation equally”, over ten thousand sick children (11, 145 to be exact) are waiting to be seen for an appointment in our public hospitals.
The main media coverage of the recent figures released from the National Treatment Purchase Fund highlighted the size of the overall waiting lists numbers, including both adults and children, which has reached almost half a million. I have analysed the waiting lists to look specifically at the numbers of children who are waiting to be seen in our hospitals. I also looked back at the figures for 2014 to see how the waiting lists have changed in this period.
Chart 1 below shows that things have worsened considerably in quite a short space of time. We can see that the numbers of children waiting over six months on day case lists has increased by three quarters (75%) from 1675 to 2944.
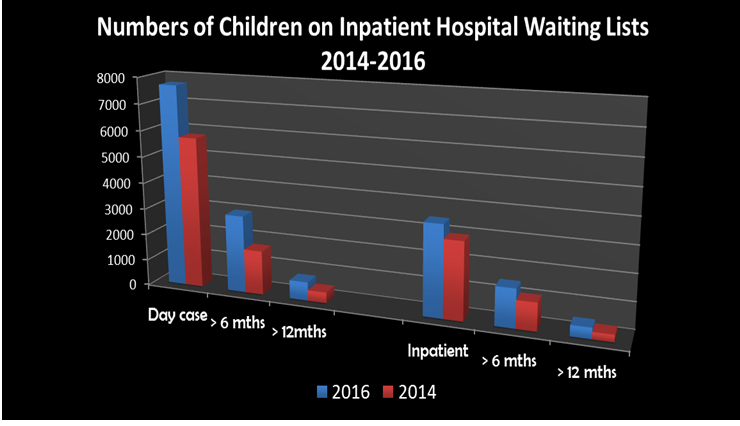
While there was an increase by 40% of children waiting longer than six months for inpatient care.
Six months is a substantial length of time in a child’s life. The waiting time can result in illnesses worsening or being undiagnosed, and the principle of ‘early intervention’ and preventative action is clearly not being achieved in these instances. It also causes significant suffering, stress and worry for children and their parents, waiting month after month and in some cases, over a year, to be seen in a hospital for illnesses relating to Ear Nose and Throat, Respiratory illnesses, Cardiology, Surgery, Orthopaedics and even Radiology.
The waiting lists differ from hospital to hospital and regionally. In Chart 2 below I have broken down the figures to show the hospitals with the highest waiting lists in 2016. We can see that for hospitals like Our Lady’s Hospital Crumlin the numbers of children waiting for day cases increased by 43%. Some of our regional hospitals like Galway and Waterford are also notable for their high waiting lists and significant increases over the last year.

The reasons for waiting lists are complex but there is no doubt that the funding reductions from austerity and the longer term failure to provide sufficient funding to our public health system is a significant contributory factor.
Indeed there has been some debate in the media recently about the “high” level of spending on our health services and the resultant claim that the system is the problem. But the system is dealing with insufficient staff numbers, closed beds (and wards in some instances), and inadequate facilities – not because of the lack of effort or capabilities from the people working in the health system but due to the under resourcing and the failure to develop a high quality universal public health system in Ireland.
If we look at the actual numbers we can see from Chart 3 below that Ireland’s spending on health as a % of GDP at 8.1% is below the OECD average of 8.9%. And most importantly only 68.5% of health spending in Ireland is public (i.e. 31.5% is private) versus the OECD average of 72.7% and countries such as the Denmark where it is 84.3% and the UK where public spending is 86.6%. This means that only 5.5% of GDP is spent on public health care in Ireland versus 7.3% in the UK.
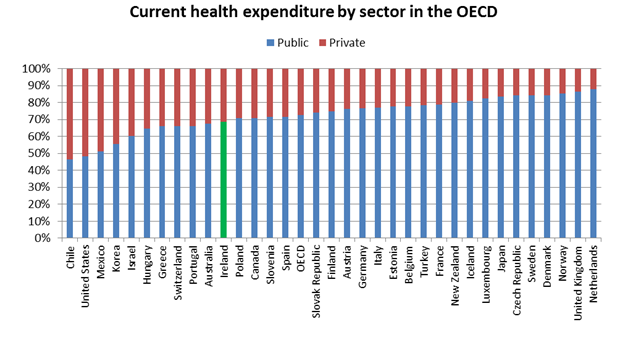
We can see then that a relatively high proportion of spending on health in Ireland is private. This means that access to health care in Ireland is strongly influenced by private individuals’ and families’ ability to afford it. The public health system in Ireland does not provide universal comprehensive accessible healthcare, like for example, the National Health Service in the UK. So in Ireland those who can afford it are likely to be buying a greater access to healthcare than lower income households in Ireland through the private hospitals and clinics (who highlight this point in their stomach-churning advertising). Also people who don’t have a medical care or health insurance are charged for use of the public system as well.
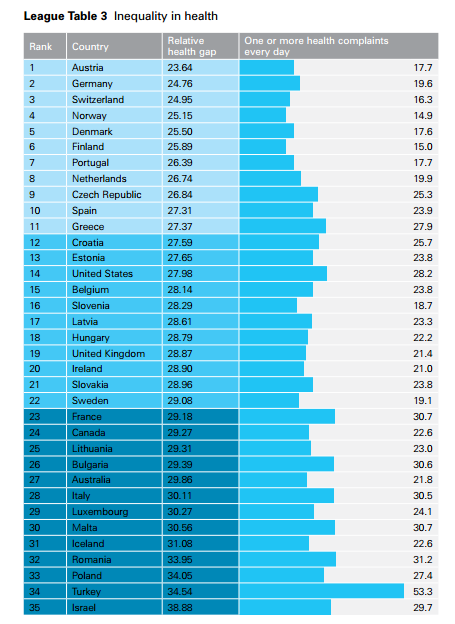
The recently published UNICEF’s "Report Card 13, Fairness for Children: A league table of inequality in child well-being in rich countries", ranks 41 EU and OECD countries for “bottom end inequality” of income, educational achievement, and self-reported health and life satisfaction. While Ireland is placed 7th out of 41 EU/OECD countries across all dimensions of inequality, the report shows that a third of all Irish children live in materially deprived households. In terms of health we can see in Chart 4 below, which is reproduced from the Report, that Ireland came 20th on a list of 35 EU/OECD countries in terms of self-reported health problems. These include psychosomatic symptoms like headache, stomach ache, feeling low; feeling nervous; difficulties in getting to sleep; and feeling dizzy.
Overall then this analysis shows that children who are reliant on the public system are left waiting for months and even years to access necessary health care while children whose families can afford it can avoid the waiting lists and access care through the private health system. This is grossly unfair and unequal. It reinforces other economic inequalities affecting thousands of children in Ireland.
The waiting lists show that we need to develop a properly funded universal public health system in Ireland that can provide equal and timely access to high quality treatment for all our citizens. The debate in the recent election pointed to a greater level of public support for such a system and the use of a sustainable tax base (such as the USC) to pay for it.
Dr Rory Hearne is a Senior Policy Analyst with TASC
Dr Rory Hearne @RoryHearne

Rory Hearne is a postdoctoral researcher in the Maynooth University Social Sciences Institute (MUSSI), working on the Re-Invest Participatory Action Human Rights and Capability project in relation to social investment with a particular focus on homelessness and water infrastructure.
He has a PhD in political and economic geography from Trinity College Dublin. He is also a former policy analyst with TASC and has worked as a policy researcher and community development worker with Barnardos on social housing regeneration and human rights in Dublin's inner city. He was lecturer in human geography in the Department of Geography, Maynooth University and has researched and published extensively in the areas of housing and social housing, political economy, human rights, social movements, and politics.
He is author of Public Private Partnerships in Ireland (2011) and co-author of Cherishing All Equally (2016). He is also a regular economic and social analyst on various national media.
Share:


