Cancer is one of the biggest health challenges in Ireland, but its impact is not felt equally across the population. Breast cancer accounts for 31.8% of all cancer diagnoses among women, while ovarian cancer represents almost 7% (NCRI, 2024). Yet, behind these national statistics lies a stark reality: where you live and your socioeconomic circumstances dramatically affect your chances of survival.
Underserved people are more likely to be diagnosed later, have poorer access to treatment and face lower survival rates. With breast and cervical cancer cases projected to rise to 113% by 2045 (NCRI, 2024), Ireland's health system faces a pressing question: how do we ensure everyone gets the care they need, regardless of location or socio-economic status?
Geography Matters
Ireland has recently been divided into six health regions: Dublin and North East (DNNE), Dublin and Midlands (DNML), West and Northwest (WNW), South West (SW), Dublin and South East (DNSE) and Mid-West (MW). People with breast cancer face dramatically different survival rates across these regions. Shown in the bar chart below, for breast cancer patients diagnosed between 2009-2018, the national five-year survival rate was 85.1% (highlighted in green). However, in the Mid-West region, that figure dropped to 80.1% (indicated by an asterisk beside the figure) (NCRI, 2024). These data show that although female breast cancer survival rates are quite consistent across regions, the 5-year survival rate is a noticeable outlier for women living in the Mid-west region, suggesting that the differences may be significant. The 5% difference may seem small, but it represents lives that might have been saved with earlier diagnosis.
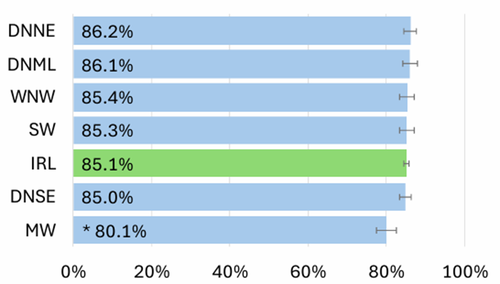
Breast Cancer (Females): Age standardised 5-year net survival percentage by region during the period 2009-2018 (NCRI, 2024).
Around 60% of all cancers occur in the more densely populated eastern half of the country, particularly in Dublin. While Dublin's health services struggle with this concentrated demand, rural areas are left underserved. The Irish Cancer Society has highlighted this shocking variation in access to cancer tests and treatments across Ireland, with patients outside major urban centres facing significantly longer wait times for diagnosis and treatment. Most alarmingly, the organisation has shown concern in the delays for patients referred for urgent breast cancer checks. These delays are particularly devastating for rural patients who may already face weeks of travel planning and financial burden just to access the tests they desperately need.
Socioeconomic Divide
Geography is only part of the story; socioeconomic inequalities play an even bigger role in shaping cancer outcomes. Research from a TASC report on Health Inequalities in Europe shows how socioeconomic factors such as employment status, income level, education, age, sex, ethnicity, gender or disability status plays a role in determining the health of individuals.
Those with greater social advantages tend to achieve better health outcomes compared to individuals from lower socioeconomic backgrounds. These health inequalities, and specifically cancer inequalities, emerge from the different exposures and vulnerabilities to health risks that exist across social groups.
The Pobal HP Deprivation Index is a social gradient tool that measures levels of disadvantage across Irish communities. It highlights a clear social gradient in cancer risks among women in Ireland. Women living in Ireland's most deprived areas face a 5% higher overall risk of developing cancer compared to those in affluent areas. For cervical cancer, the disparity is even starker as women in the most deprived areas face an 84% higher risk compared to those from affluent areas (Bambury, 2023). The survival gap is equally concerning, between 2014 and 2018, women from the most deprived areas had significantly poorer five-year survival rates across multiple cancers, including breast cancer compared to those in affluent areas (Bambury, 2023).
These statistics reveal a healthcare system where geography and economic circumstances create a two-tier cancer experience, one for the affluent and well-located, another for the disadvantaged and isolated. This socioeconomic divide creates barriers at every stage of the cancer journey, from late detection to inadequate treatment access.
Why Cancer Inequalities Exist
The National Cancer Strategy 2017–2026 includes a commitment to reducing health inequalities, this aligns with Europe’s Beating Cancer Plan which sets a goal for Europe to improve cancer care and reduce inequalities. Yet, women’s cancer outcomes in Ireland continue to be shaped by a complex mix of systemic, cultural and economic factors.
1. Barriers to Early Diagnosis
Evidence consistently shows that early-stage cancer diagnosis dramatically improves survival rates. However, uptake in screening services remains low among women living in deprived areas and immigrant communities across Ireland (Bambury, 2023). Immigrant communities refer to groups of non-residents arriving in a state with the intention to remain for a period exceeding a year.
Low participation in screening can stem from various challenges at the individual level. For example, limited health literacy and awareness prevent many women from recognising cancer symptoms or understanding the benefits of regular screening.
A recent TASC report on Migrant Communities Needs Assessment, gave an insight into how these individual level challenges can be more prominent for immigrant women because of language difficulties, cultural stigma surrounding cancer and limited understanding of healthcare entitlements in Ireland. These factors result in immigrant women missing opportunities for early diagnosis (TASC, 2025).
Beyond individual challenges, structural inequalities within the healthcare system create additional obstacles. Deprived and rural areas face significant GP shortages, while access to diagnostic services within the public system remains inconsistent. Extended waiting times for specialist services further contribute to delayed diagnoses, particularly affecting women who cannot afford private healthcare options (National Cancer Strategy 2017- 2026 & TASC, 2022).
2. Financial Burden
Cancer imposes financial costs that can deter women from seeking care or interrupt their treatment.
Direct healthcare costs include some of the following, over the counter/prescription medication, GP visits and consultant appointments. However, indirect costs often can be more burdensome, some of these include a loss of income from work absences, ongoing household expenses such as mortgage payments and utilities, childcare arrangements and transportation costs including parking fees, taxi fares and public transport (TASC, 2022).
Economic circumstances often interact with geographical distance, creating a double burden where rural and immigrant women face reduced healthcare access due to limited nearby services and inadequate or a lack of transportation options (TASC, 2025).
3. Culture and Language
Language barriers significantly reduce participation in cancer screening programs among immigrant communities who are not proficient in the dominant language. Limited proficiency is made worse by a lack of translated resources and limited interpreter availability within health services (TASC, 2025). TASC researchers have found that inadequate translation materials and interpretation services have negatively impacted both access to and the quality of services.
Cultural factors further complicate matters. Some communities maintain beliefs about the danger of naming cancer, while others attach stigma to screening procedures. These barriers result in reduced screening participation and delayed diagnosis for some immigrants, while others seek a higher standard of affordable preventative care services abroad (TASC, 2025).
4. Psychological Barriers
The emotional impact of cancer diagnosis and treatment creates additional barriers to seeking cancer care. Psychological responses including fear, shame and fatalistic attitudes can lead to avoidance behaviours, causing women to ignore or delay checking symptoms (TASC, 2022). These psychological barriers are particularly pronounced among women who have witnessed poor cancer outcomes in their communities or who hold cultural beliefs about cancer as an inevitable or shameful condition (TASC, 2025).
The Path Forward
Addressing these disparities in cervical and breast cancer care require tackling their root causes.
1. Reduce Financial Burden
Measures have been taken to alleviate some of the financial burden of travel costs with the Travel2Care scheme, run by the Irish Cancers Society, which offers transportation assistance to aid patients travelling to cancer centres. Additionally, steps are being taken for cancer survivors to have the “Right to Be Forgotten.” This refers to having past cancer diagnosis disregarded when accessing financial services like mortgages and insurance as cancer survivors face higher premiums as a result of their health history.
However, additional financial support measures could further reduce barriers to care. In order to influence the next national budget, The Irish Cancer Society’s pre-budget submission identifies key areas where targeted investment could make a real difference. Some of their suggestions include abolishing car parking charges for cancer patients at healthcare facilities and providing automatic medical card eligibility for all cancer patients from diagnosis through treatment completion.
2. Increase and Expand Awareness
In order to make more of the population aware of the signs and symptoms of cancer there needs to be an investment in public awareness campaigns (TASC, 2025). One such measure that Ireland has taken is The Traveller Health Project which addresses cancer prevention and early detection, providing screening information to Travellers in the Finglas and Blanchardstown suburbs of Dublin. As part of this programme, primary healthcare workers received training to deliver BreastCheck messages to these communities.
Similar culturally appropriate awareness campaigns should be extended to rural communities and other marginalised groups across Ireland. Investment in nationwide public awareness campaigns would ensure that knowledge of cancer signs and symptoms reaches all corners of the country, particularly in areas where access to healthcare information may be limited.
3. Make Information More Accessible
The National Screening service has taken steps towards language inclusivity by creating videos messages in 25 languages on screening programmes for immigrant communities, including Breastcheck and CervicalCheck videos.
However, there is still a lot of room for improvements to be made to ensure full inclusivity and accessibility. TASC's report on Migrant Communities Needs Assessment puts forward the recommendation of widening translation services, including plain English documents and websites that fully match their English counterparts. Information should be made available in multiple formats such as audio, video and captioned content to address varying literacy and numeracy levels across communities.
Furthermore, the use of interpreters is another way around language barriers. At present in Ireland and other EU countries there are several barriers that have prevented interpreters being widely used, such as a limited number of qualified interpreters, restrictive legislation and policies and the financial costs (Vange et al. 2024). An article in RTE supports evidence found in TASC’s Migrant Communities Needs Assessment report by highlighting how it is the common case in Ireland that family members, friends and in come cases the children of patients are being used as an interpreter. This results in some children missing school or information not being relayed properly.
Additionally, for people with disabilities, addressing communication barriers and improving physical accessibility at screening sites remains a priority. Common physical barriers include no ramps and inaccessible examination rooms and equipment. It is often the case when people with a disability arrive for screening staff are inadequately prepared to accommodate their needs (Lezzoni,2022).
4. Invest in Health Infrastructure
Ireland’s cancer screening programmes represent an important part of its healthcare system by providing early detection services. Yet, despite such efforts, The European Cancer Inequalities Registry reveals that Ireland continues to lag behind other European countries when it comes to our overall standard of healthcare infrastructure. This has prompted the Irish Cancer Society in its Pre-Budget Submission 2026 to emphasise the need for increased investment in physical infrastructure, as cancer care services currently compete with other health services for limited resources.
Additionally, Ireland’s two-tier health system exacerbates existing disparities. Evidence has shown that patients with health insurance are more likely to have an earlier cancer diagnosis, have access to better standards of cancer treatments and as a result have better overall survival rates. Patients without insurance are more likely to have poorer survival rates and less likely to participate in screening programmes. Along with these patients are faced with long waiting times for diagnostic tests and inadequate access to newly available cancer drugs (Killian et al. 2023). Killian and colleagues (2023) also noted that there are issues of overcrowding, bed availability, staffing and funding. These issues are potential causes for delays in diagnosis, which disproportionately affect those who cannot afford of possess health insurance. In response the Irish Cancer Society’s Pre Budget Submission 2026 calls for an end of the widening gap between cancer patients who possess health insurance and those who do not.
Overall, cancer inequalities in Ireland reflect broader patterns of social and geographic disadvantage that demand urgent action. While progress has been made, stark disparities between regions and socioeconomic groups reveal a healthcare system failing its most vulnerable citizens. Only through reform such as investing in health infrastructure, ensuring inclusivity and accessibility in information and services, heightening awareness campaigns and removing financial barriers can Ireland ensure that cancer survival depends on the illness itself, not on where you live or your social status.
References:
Bambury, N., Brennan, A., McDevitt, J. & Walsh, P.M., 2023. Cancer inequalities in Ireland by deprivation, 2004–2018: A National Cancer Registry report. Cork: National Cancer Registry Ireland.
Iezzoni, L.I., 2022. “Cancer detection, diagnosis, and treatment for adults with disabilities”. The Lancet Oncology, 23(4), pp.164- 173.
Irish Cancer Society, 2025. Pre-budget submission 2026. Dublin: Irish Cancer Society.
Killian, M., O’Mahony, D., Murphy, K., O’Connor, D., Bird, B. & Murphy, C.G., 2023. “Breast cancer outcomes in a private hospital appear better than national outcomes in a country with a mixed public/private healthcare model”. Irish Journal of Medical Science, 192(2), pp.527–531.
National Cancer Registry Ireland, 2022. Cancer trends: breast, cervical and colorectal cancer 1994–2019. Cork: National Cancer Registry Ireland.
National Cancer Registry Ireland, 2024. Cancer in Ireland 1994–2022: Annual statistical report of the National Cancer Registry. Cork: National Cancer Registry Ireland.
Department of Health, 2017. National Cancer Strategy 2017–2026. Dublin: Department of Health.
TASC, 2018. Health inequalities in Europe: Setting the stage for progressive policy action. Dublin: TASC.
TASC, 2022. Understanding the challenges of cancer and socio-economic inequality in Ireland. Dublin: TASC.
TASC, 2025. Migrant communities needs assessment: Examining the experience of migrant communities in seeking access to cancer and healthcare services. Dublin: TASC.
Vange, S.S., Nielsen, M.R., Michaëlis, C. & Smith Jervelund, S., 2024. “Interpreter services for immigrants in European healthcare systems: a systematic review of access barriers and facilitators”. Scandinavian Journal of Public Health, 52(7), pp.893–906.
Clodagh Lynch

Clodagh Lynch is a master's student in Politics and Data Science at UCD. Additionally, she holds as a BA in History and Politics from UCD. As part of summer semester, she is interning at TASC in the health stream. She has a personal interest in providing data-driven solutions to policy challenges through quantitative analysis and evidence-based research.
Share:


